
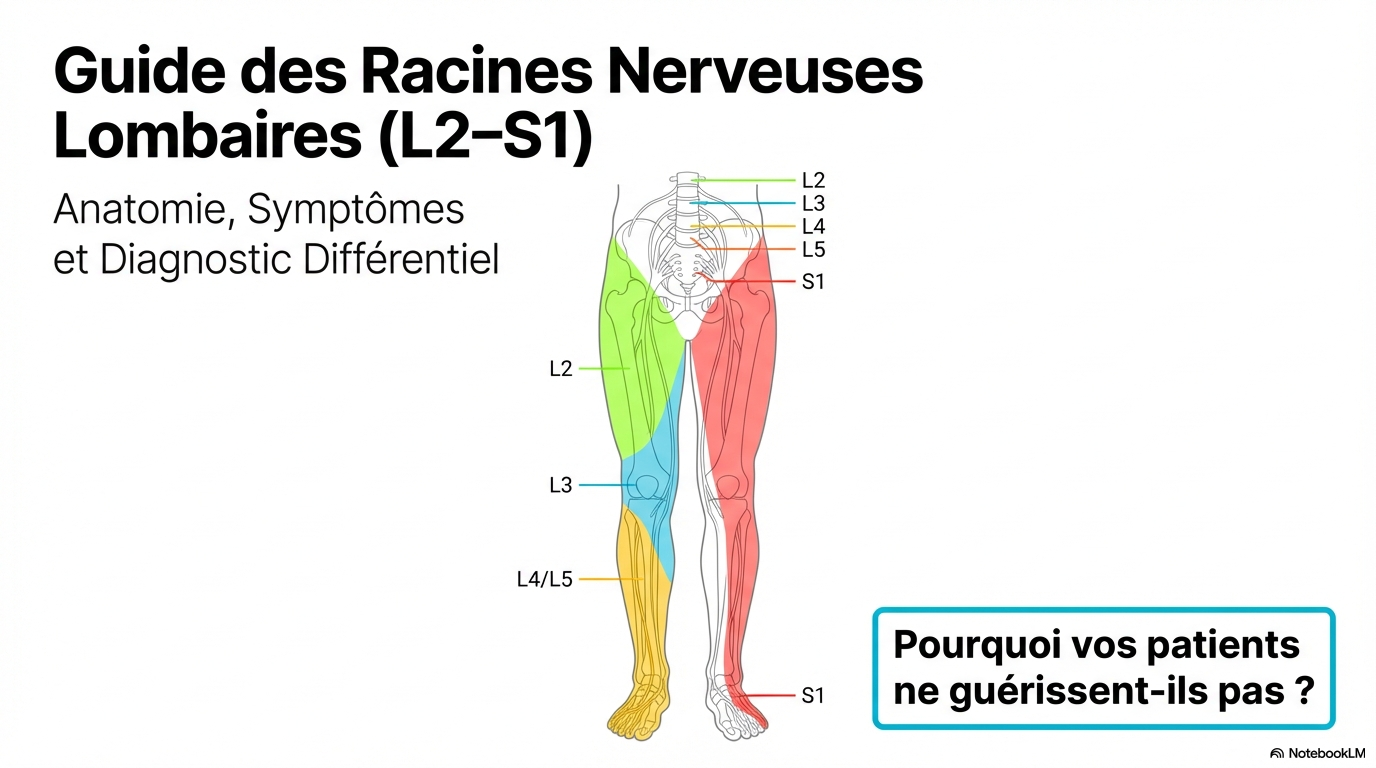
Knee pain?
The problem might be coming from your back.
Are you receiving treatment for patellofemoral pain syndrome, tendinitis, or a torn meniscus without lasting success? This is often because the true cause is in the lumbar region. Discover how nerve compression radiates to the knee and destabilizes the joint.
The "Fake" Knee Problem
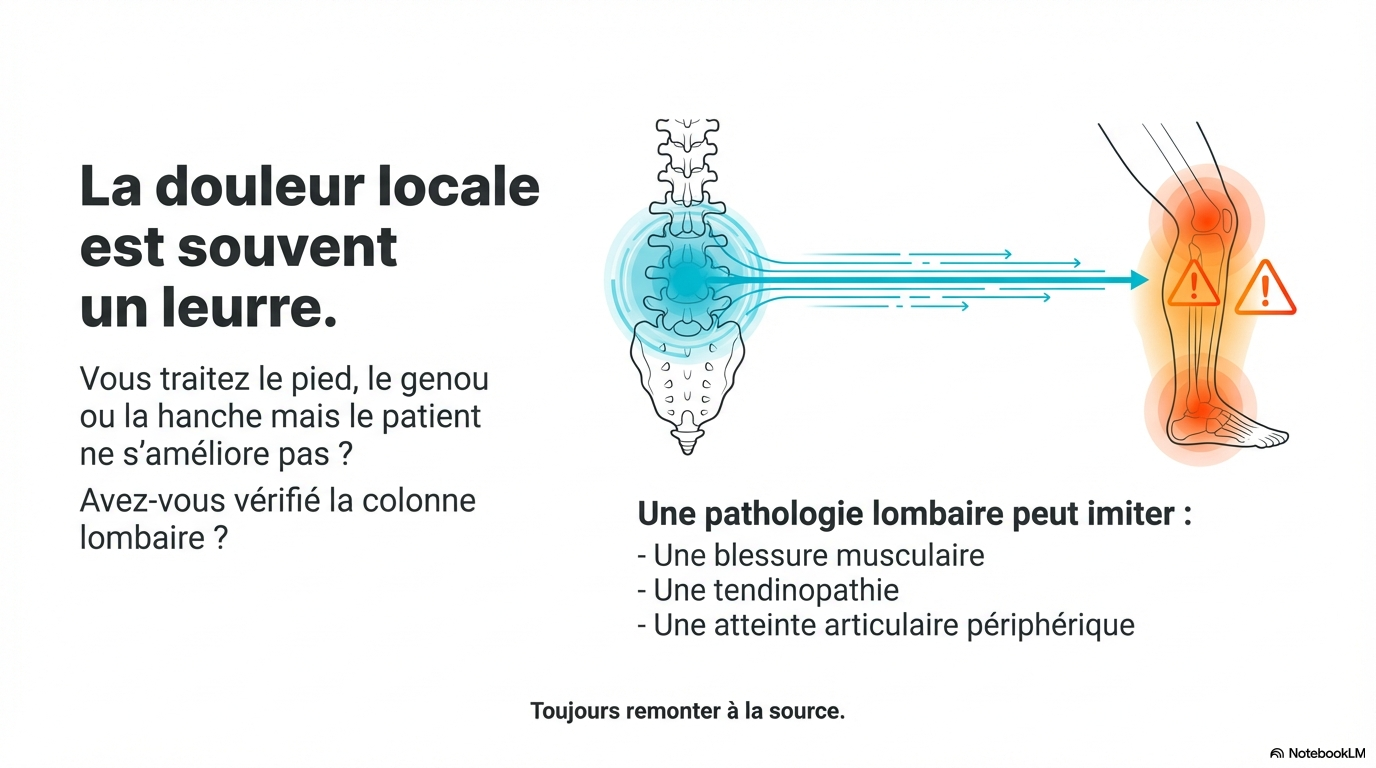
To persist in treating the knee joint with injections or knee braces when the femoral nerve or sciatica Pinching in the lower back is a very common diagnostic error that hinders your recovery.
Anatomy & Pathology
The impact of the lumbar nerves on the knee
The pain you feel on, around, or behind your kneecap very often comes from a herniated disc lumbar which sends a "false signal" along the leg.
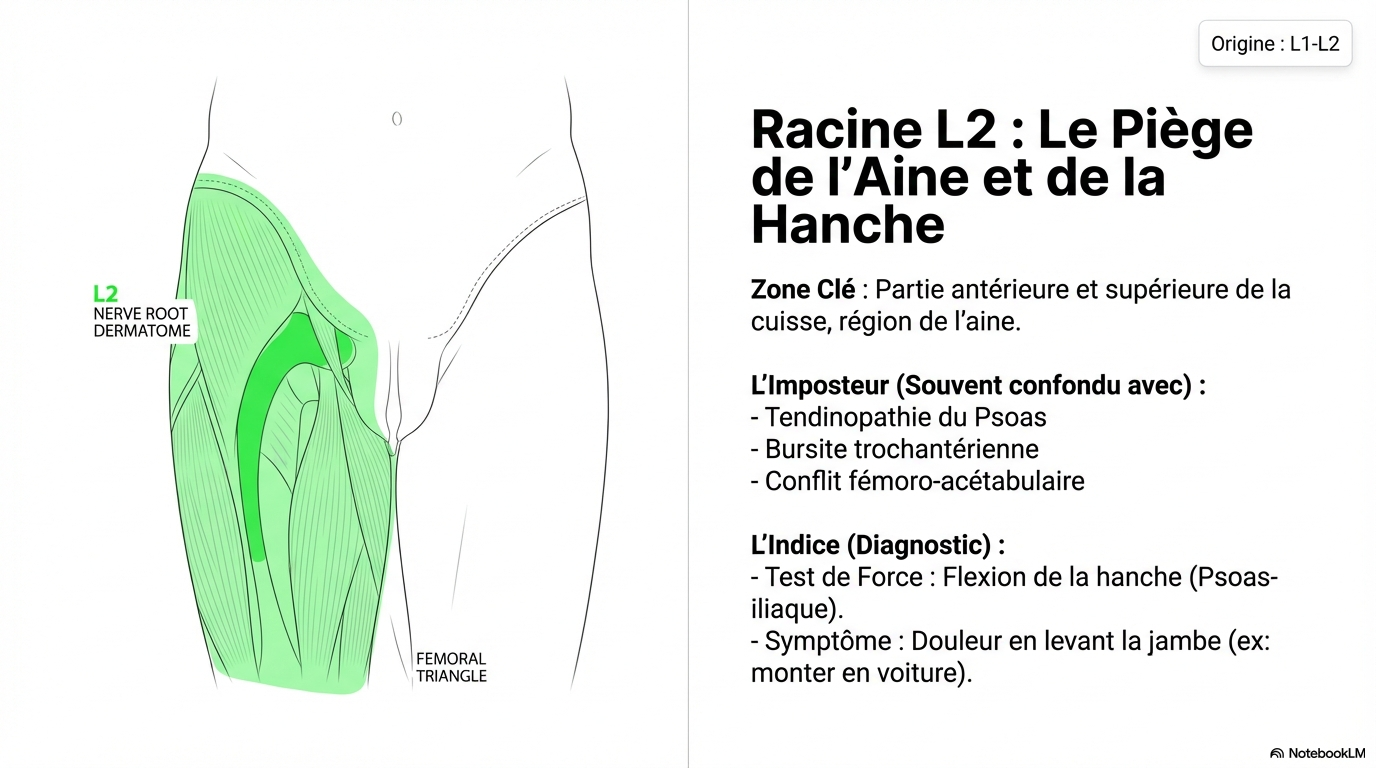
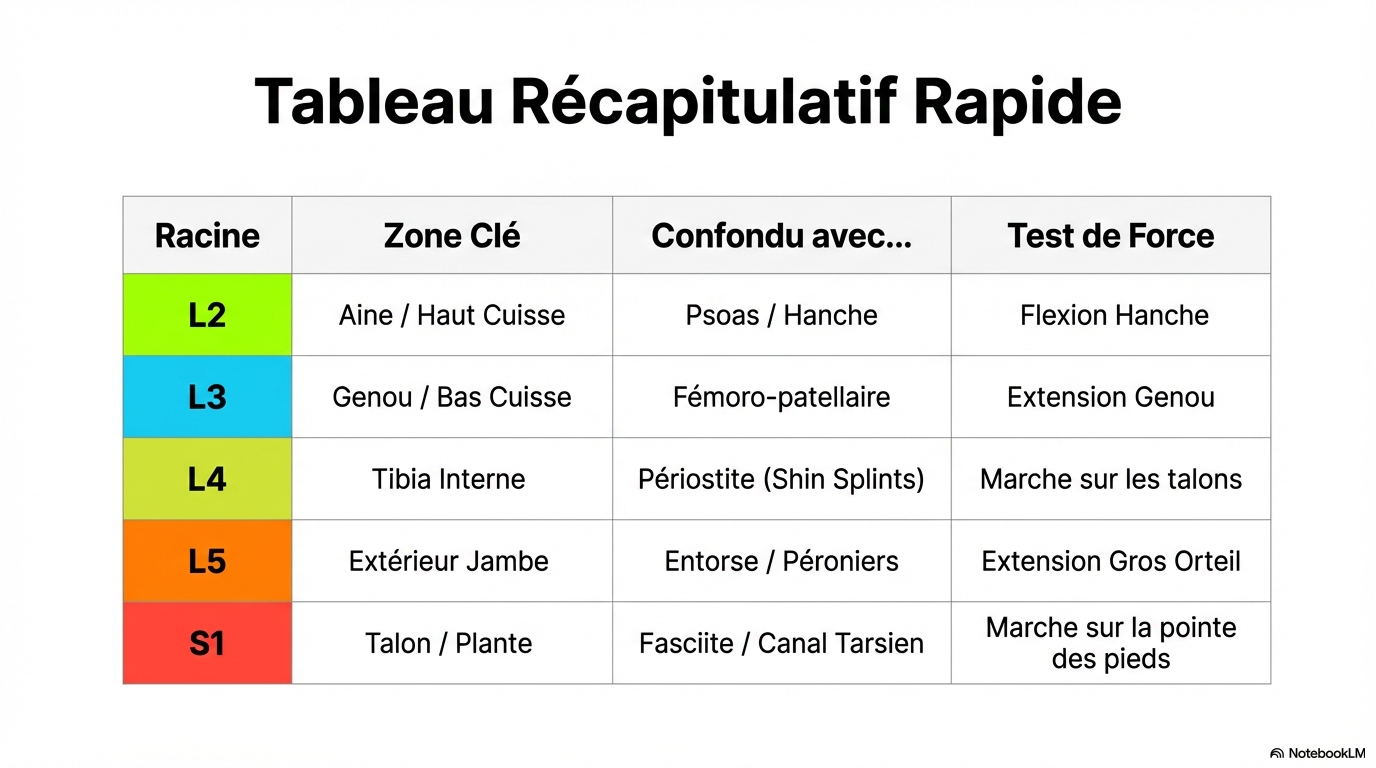
Root L2
Origin: L1-L2upper thigh
(Psoas, flexors)
Sensory Zone
Upper thigh • Groin
Referred pain
The pain radiates down the front of the thigh but usually stops well before reaching the knee. It is less frequently associated with purely knee-related pathologies.
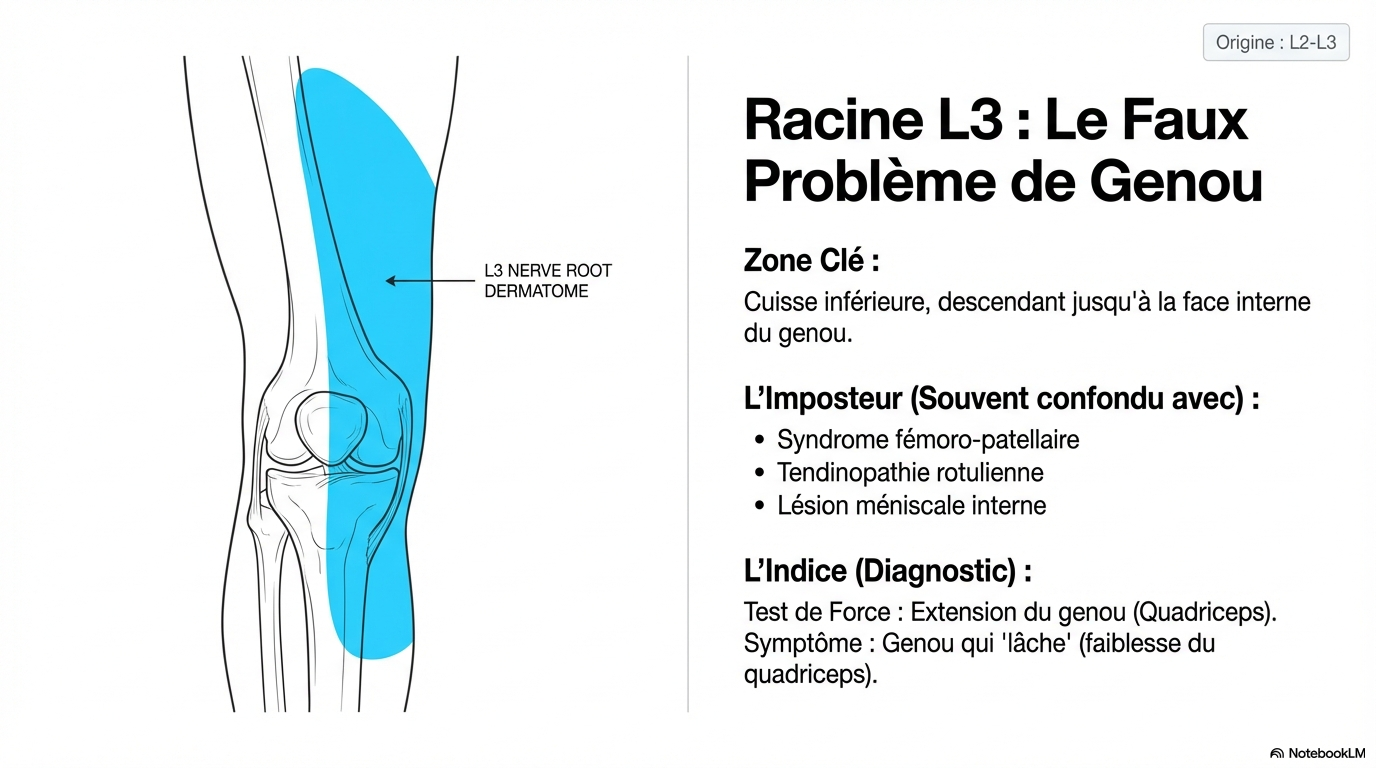
Racine L3
Origin: L2-L3Quadriceps Control
(Anterior thigh muscle)
Sensory Zone
anterior surface of the descending thigh just above the kneecap
Quadriceps tendinitis?
It often mimics inflammation of the tendon above the knee. A pinched L3 nerve root causes a feeling of heaviness in the thigh and pain at the top of the joint.
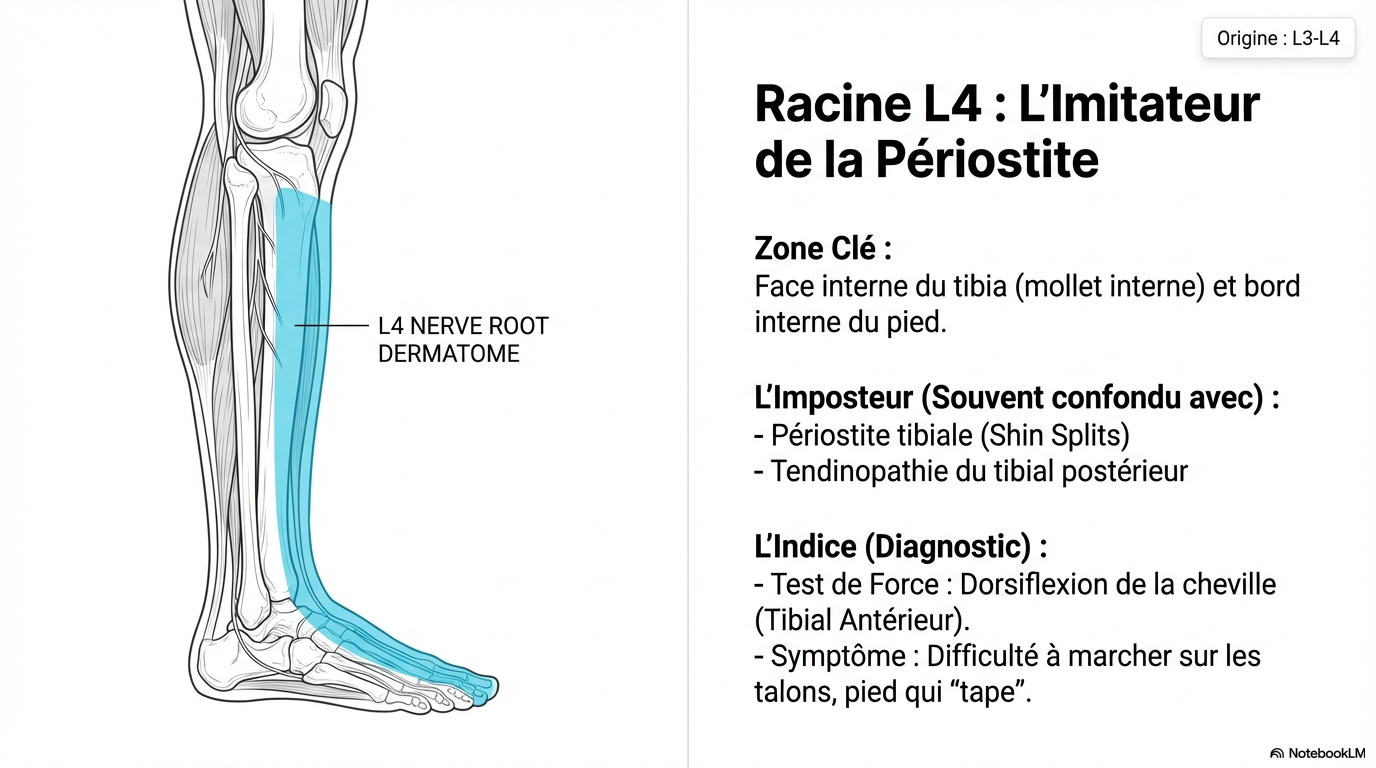
Root L4
Origin: L3-L4Knee Extension
(Patellar tendon, patellar reflex)
Sensory Zone
On and below the kneecap • Inner surface of the tibia
The Great Mime
Often confused with patellofemoral pain syndrome, medial osteoarthritis, or patellar tendinitis. If the knee "gives way" when going down stairs, L4 is the prime suspect.
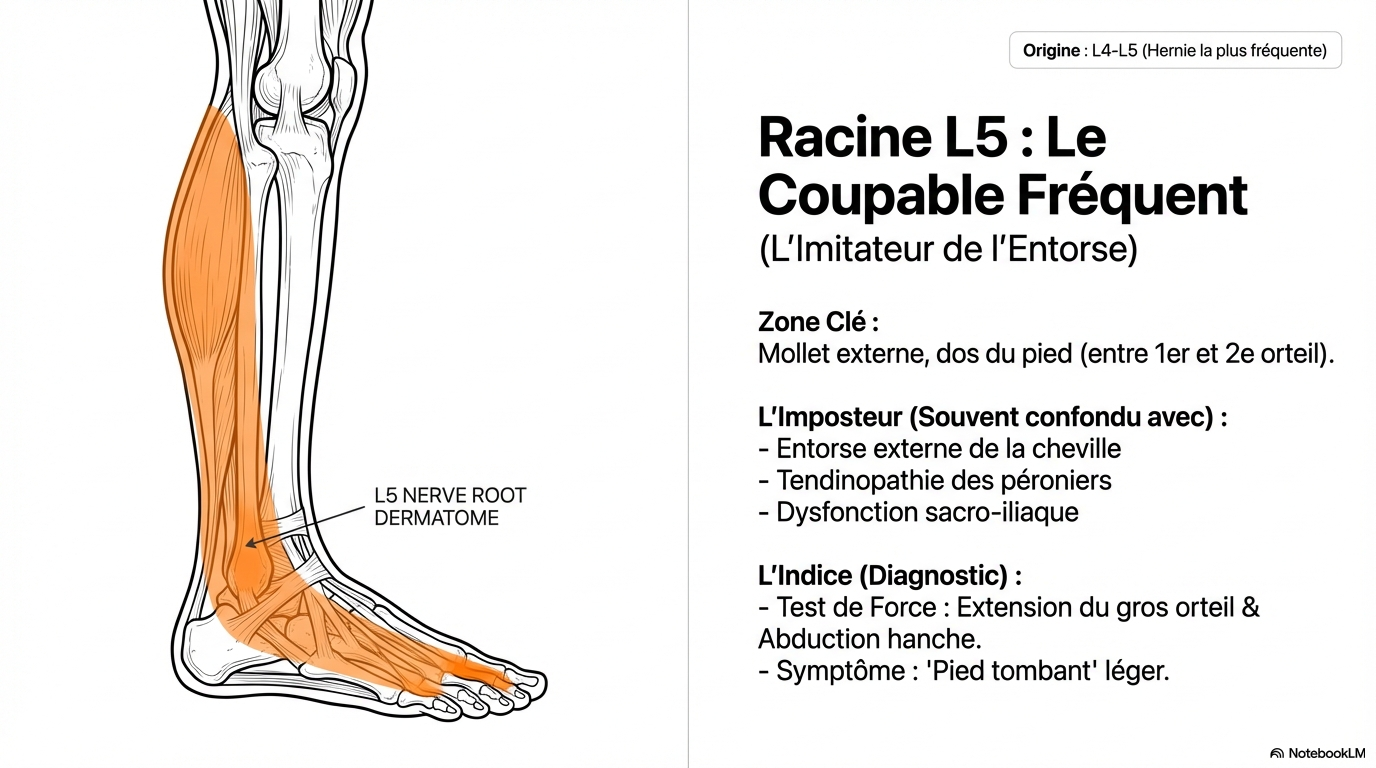
Root L5
Origin: L4-L5Lateral Stability
(Gluteal stabilizers, peroneal muscles)
Sensory Zone
Outer thigh • Outside of the knee • Outer part of the calf
Windshield Wiper Syndrome
Pain on the outer side of the knee in runners is often diagnosed as IT band syndrome, but may be a hidden L5 radiculopathy.
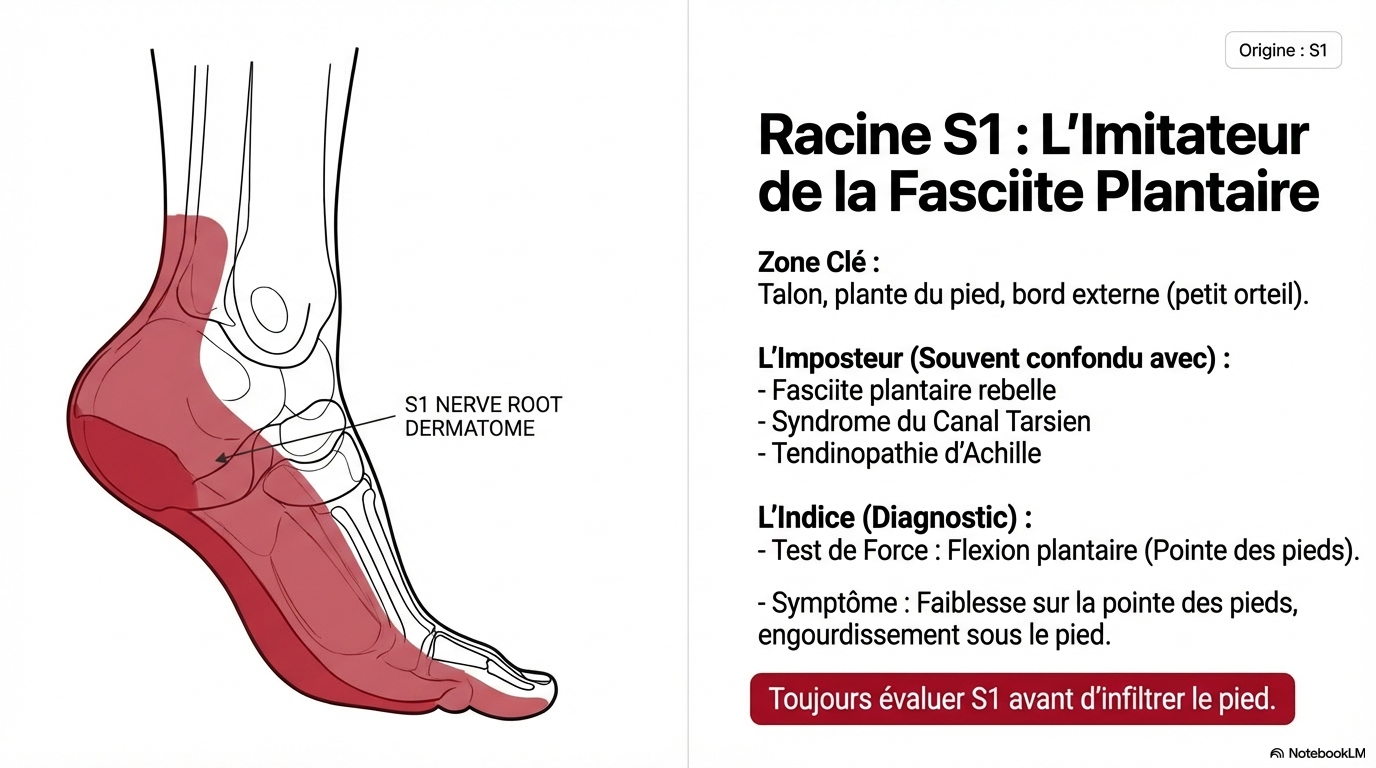
Root S1
Origin: L5-S1Knee Bending
(Hamstrings, Calves)
Sensory Zone
Buttock • Back of thigh • Hollow behind the knee
Baker's cyst
A constant pain or tension behind the knee (popliteal fossa) is often the direct manifestation of the sciatic nerve irritated at the S1 root.
Differential Diagnosis
Knee or Lower Back? (Or both?)
To avoid unnecessary meniscus surgeries, it is imperative to determine the exact origin of the pain through a thorough clinical evaluation.
How do we make the diagnosis?
MRI (Knee vs. Lumbar)
Knee MRIs very often show benign lesions (normal age-related wear and tear of the meniscus) that are not the true cause of the pain. lumbar MRI is often necessary to identify a stenosis or herniation (L3-L4) that projects pain onto the knee.
Neurological Provocation Tests
We carefully assess your patellar reflexes (L4 nerve). Most importantly, we practice the Femoral nerve stretch test (PKB). If stretching the nerve in your back reproduces the pain in the front of your knee, the origin is lumbar!
The Domino Effect (Coexisting Pathologies)
Sometimes the wear and tear on your knee is real, but it has been provoked and accelerated due to a problematic back.
The cascade of destruction:
- 1. L3-L4 lumbar herniated disc
- 2. Decrease in the electrical signal to the quadriceps muscle
- ↓
- 3. Ball joint misalignment (the ball joint is not rubbing properly) = Local osteoarthritis and inflammation
Why is local physiotherapy stagnating?
You can do all the knee strengthening exercises possible, but if the nerve (the "electrical wire") is pinched in your back, the quadriceps muscle will not activate properly to stabilize your knee when walking.
Consequence: Treating the knee alone is insufficient. To protect your joint in the long term, you must first "reconnect" the quadriceps by releasing the lumbar nerve root using the Spinal decompression therapy.
The Solution: Spinal decompression therapy
To the TAGMED CLINIC, We target the true source of your knee instability and pain. If your symptoms stem from femoral or sciatic nerve pain, local knee treatments will only offer temporary relief.
The lumbar neurovertebral decompression is an advanced, non-invasive technology. By creating a computerized and specific stretch of the lower back, it generates negative intradiscal pressure. This shrinks herniated discs, rehydrates worn discs, and releases the nerves (L3, L4, L5) that control and protect your knee.
Effective for treating lumbar causes of knee pain:
- L3-L4 radiculopathy mimicking patellar pain
- Unexplained quadriceps muscle weakness ("knee giving way")
- Foraminal stenosis strangling the femoral nerve
- Sciatica radiating into the popliteal fossa (behind the knee)
- Lumbar disc herniations and bulges (L3 to S1)
Do not treat the symptom.
Address the root cause.
Failure of local treatments (knee injections, taping, knee braces, surgery minor meniscus...)
Specialized lumbar assessment (L2-S1) by a spine expert
Lumbar Neurovertebral Decompression
Nerve release, return of patellar muscle control and cessation of knee pain.
Stop the progression of your knee pain.
Let's check the condition of your lumbar nerves today to put your mind at ease.

